SUPPLEMENTAL ENTRY:
OPEN LETTER TO WAMES AND CLWYD SUPPORT GROUP
How are WAMES and Clwyd group going to contact the hundreds and hundreds of N Wales ME/FM patients who have been mucked up by these psych-Clinics for the last ten years, put right the "harm" the latest enclosed Report notes (Twisk-Maes, 2009), and then explain to those individuals that the Support groups were told what was happening years ago and yet they never challenged the Service directly once with so much as a simple letter asking, for example, if the Clinics accepted the WHO ME/CFS definition? That would have nailed their stance easily and defined any patient-advisory position we had in Wales toward the 'Service' instantly and forever. (We know because we did ask the NHS Clinics).
But on the contrary Clwyd Group are currently promoting not only their own but OUR NW Wales damned CBT/GET ME/FM Clinic as well on their web site, and to the ME Association, even as this email is sent out.
A lot of people think the only damage that has ever been done to ME/FM patients was via the efforts of the psychiatric industry, but the latter also sought and certainly found its various and incidental accomplices: Our web pages will continue to recount the history of what has transpired here in Wales over the last decade.
In the meantime, will the mid-Wales, WAMES and Clwyd Newsletters, and web sites, now attempt to contact the many "harmed" Welsh patients described in Twisk and Maes and explain fully to all how that damage has come about, been maintained, and continues to be the case (as Clwyd web page demonstrates) with ME/FM patients in Wales, and after all these years?
Karl Krysko.
9oct28
(ends)
The Report sent was:
"A review on cognitive behavorial therapy (CBT) and graded exercise therapy (GET) in myalgic encephalomyelitis (ME)/ chronicfatigue syndrome (CFS):
CBT/GET is not only ineffective and not evidence-based, but also potentially harmful for many patients with ME/CFS."
Authors: Frank N.M. Twisk and Michael Maes
Journal: Neuroendocrinol Lett 2009; 30(3):
284=96299 PMID: 19855350 NEL300309R02
North WALES CBT/GET post-CLINIC PATIENTS:
This study makes it very clear that some of the most recent and state of the art means of assessing CFS (ME/FM) patients following exertion implies directly that GET ‘amplifies’ molecular and biochemical abnormalities ‘already present’ pre-exercise. This will be aggravated to an extent that is either clinically presenting (with symptoms) or sub-clinically (without overt symptom amplification).
Given that the doctrine taught at these Clinics is to elevate levels of activity, which is to be maintained thereafter over time indefinitely, the damage being done to the already compromised biological systems identified in Twisk and Maes, and exacerbated by GET, effectively becomes ‘self’- induced (by the patient themselves), protracted and accumulatively serious, potentially, disrupting those offset health systems, such as the immune, neurological and vascular, even further had they not been prescribed GET methods.
While the damage only begins at the CBT/GET Clinic, it can thus be maintained by the patient years beyond, especially for those in whom the treatment does not induce a major relapse anyway and who make that connection. Infact, ME/FM patients are 'better off' making such an early realization.
Because we have two ME/FM CBT/GET and one FM Clinic situated geographically in close proximity, in a relatively high populous area, and existing over ten years, the north Wales coast probably has one of the highest densities of post-Clinic ME/FM casualties in all Britain.
9nov01
ITEM TO BE UPDATED IN LIGHT OF A FURTHER WELSH CFS/ME FM CBT/GET RESIDENTIAL CLINIC IN MID-WALES AT BRONLLYS HOSPITAL.
______________________________
Presently, two web pages advertise both the CBT/GET N Wales Clinics noted above. One is the ME Association and the second is in N Wales itself.
Copied currently from their own web page http://www.clwydme.net the following description and contact details have been taken directly from that source (click the home page 'Update on Services in North Wales):
N Wales ME Clinics CFS/ME Services in North Wales
There are two programmes in North Wales currently providing services to assist sufferers in their management of their CFS/ME. These are based at Connah’s Quay Clinic in Deeside, receiving referrals from the east of North Wales, and Eryri Hospital in Caernarfon taking referrals from the west. The campaigning of our support group played a large part in the NHS setting up these clinics.
Referral to the services is via the individual’s own GP after they have diagnosed CFS/ME. They should write to:
ME/CFS Service,
Connah’s Quay Clinic, Wepre Drive, Connah’s Quay, Deeside, Flintshire CH5 4HA.
Tel: 01244 813486
or
ME/CFS Service, Peblig Ward, Eryri Hospital, The Park, Caernarfon, Gwynedd. LL55 2YE.
Tel: 01286 662734
The schemes are both multidisciplinary, with input from General Practice Physicians, Clinical Psychologists, Dieticians and Physiotherapists. The programme involves attending eight group sessions, on a weekly basis, where the sufferer is coached in various skills to assist in managing the condition with the hope of gaining sufficient control over symptom fluctuation to improve function and quality of life.
This information was updated in January 2008 for further information please contact one of the clinics at the addresses above.
The ME Association information page is much the same giving identical contact details to patients but it also indicates that their information advertising the Clinics has been passed on from another source. It reads:
ME/CFS services in North Wales
We have been given the following information about NHS services for people with ME/CFS in North Wales. A referral from the patient's GP will be required to access them.
We understand that both services are multidisciplinary with input from General Practice Physicians, Clinical Psychologists, Dieticians and Physiotherapists. The management programme involves eight group sessions dealing with different aspects of management.
We would welcome details for publication about any further NHS services in Wales for people with ME/CFS.
What is notable here is that at least one of these ME/CFS Suport Groups are fully aware that both of the Clinics are CBT/GET services for our patients.
And that at least one of these Support Groups knows also that CBT/GET is potentially detrimental to many ME/CFS and FM patients.
Here, for example, is the direct representation of a petition page recently removed from the Clwyd web site noted above. The wholly correct aspect highlighted in red is our emphases:
"ME-is-real e-petition to the Prime Minister.
The ME-is-real petition - response from the Prime Minister's Office.
A petition has been sent to 10 Downing Street using their e-petition facility. 8,481 people signed the petition which urged the Prime Minister to get the Health Service and medical profession to accept the WHO classification of ME/CFS as an organic neurological disorder and not as a psychosocial syndrome.
It went on to say that the latest DWP Guidelines and PACE are still directing the Health Service to treat ME suferrers with GET and CBT (a tool used for mental illnesses) despite the mounting evidence from a vast amount of research proving that ME is an organic not a psychosomatic disease and that the treatments forced onto those affected do in fact cause more harm than good and can worsen the condition of patients. Money should instead be invested in research into the physiologocal aetiology of ME/CFS and its treatment. Patients should not be forced into becoming psychiatric cases or lose their benefits.
The Prime Minister's Office has responded to that petition and you can view it at"
http://www.pm.gov.uk/output/Page14656.asp
The following is an important and illustrative example of other inherent contradictions with the above in a further extract from:
Clwyd Group ME Newsletter.
15th Birthday, 2007 Edition.
"From the Editor" (page 2)
"Just a note of clarification. ME CLWYD SUPPORT GROUP has received some criticism of our supposed support of our local NHS ME clinic. For your and others information, yes our Chairman Barbara Turnbull did on our groups behalf campaign for an ME Clinic/NHS help for patients.
What happened is that the NHS did set up this clinic, they controlled the funding and what professional help was offered, the group never had any control over this or the funding. Like other clinics in Wales it is not diagnostic and follows the NHS line of CBT therapy and physiotherapy.
Open and civil communication with the clinic should not be interpreted as blanket support. WAMES has presented a fact based Report [More Tortoise than Hare, March 2007] on Local Health Boards provision of care to ME patients, to the Welsh Assembly, outlining the dismal and poor facilities provided to ME patients in Wales....
Unlike some we do not see attacking an individual local clinic as constructive, instead we will support WAMES national push to the Welsh Assembly to update and improve the care of ME patients in Wales.
Hopefully getting them to listen to the patients rather than NICE’s new guidelines which are stuck in the psychological model, instead of the biomedical one, which is the one finding more research based evidence about ME."
This web site will be posting several important corrective points regarding this key Editorial, and other items, over the coming months.
(‘WAMES’ in this item is the Welsh Association of ME/CFS Support, and we shall be referring to them often also in this review history of the Welsh ME Service provision over the last 10 years).
9aug23
...................................................................................................................................
CLWYD CLAIM THAT THE CANADA PROTOCOL IS BEING USED BY THE TWO CBT/GET CLINICS
Up until the summer of 2009 the Clwyd Web site included information on Diagnosis, Assessment and the Canadian Clinical Working Case Definition for CFS/ME, located within the above page noted here advertising the contact addresses and program information for the CBT/GET Clinics.
Under ‘Diagnosis’ the claim is made that, ‘a diagnostic routine must be conducted prior to referral to the Clinics and involves taking a history of the patient’s health status, performing a physical examination, and imposing a battery of blood tests (including FBC, CRP, LFT, Thyroid and so on). And further tests could be initiated if there are indications to do so.’
The heading ‘Assessment’ then suggests that:
"When the referral is received the individual will be placed on the waiting list for assessment for the program, and informed in writing that this is the case. As their name comes to the top of the list they will be contacted to arrange a mutually convenient time and date to attend for assessment.
The assessment serves to confirm the diagnosis, using the Canadian criteria (described below) as guidance, as well as to explain in more detail about the program content and enable the individual to make an informed choice as to whether it would be suitable for them or not."
The final heading, ‘Canadian Clinical Working Case Definition for CFS/ME’ lists six of the criteria by which the protocol identifies hallmark features of ‘CFS/ME’ including Fatigue, Fatiguability, Sleep, Pain, Cognitive, Pain and ANS complications.
The Clwyd page concludes noting that, ‘the information sent by the Clinics was updated as of January 2008.’
Sandwiching this information between details for contacting the N Wales Clinics for referral, the Clwyd web notification therefore suggests that the NHS CBT/GET Service is complying with the essentially neurological Canada Diagnostic and Treatment Protocol.
WE DOUBT THIS VERY MUCH INDEED, and wonder how such an arrangement could ever be possible when Bruce Carruthers, the Protocol's principal author, told us delegates to the London Invest in ME Conference two or three years ago that ‘patients in the UK should actually be suing these CBT Clinics’ (and presumably their promoters), and Professor Hooper the following year noted that the CBT Clinics are a case where ‘no loaf whatever is very definitely better than half a loaf.’
While many of the ‘Diagnosis’ routines here suggested have been tried on ME/CFS FM patients for many years and are usually completely unrevealing, making it entirely ‘safe’ for the Welsh CBT Clinics to comply with them, and the ‘Assessment’ routine similarly changes nothing, the Clwyd promotion, that The Canadian Protocol is being adhered to, is hugely misleading.
Do the Clinics agree that a key diagnostic requirement for ME patients is a SPECT scan. Do the Welsh CBT Clinics comply with the views of the Protocol regarding its Treatment recommendations, or its counter-indication statements regarding the use of CBT and GET for ME and FM patients, for example?
The Clwyd information would seem to be deceptive indeed, and we wonder if that’s why, with some prompting from ourselves, it has been withdrawn suddenly and of late from their site.
But we have retained a copy of the web page, and would point out that precisely the same information is also available in print on page 19 of the Clwyd Newsletter as of Spring 2008, and has apparently therefore been misleading ME/CFS FM patients across N Wales for many months.
9aug30
......................................................................................................................................
ENTER THE 'IMSCAR' RESULTS
Toward the end of last year we contacted Clwyd Support Group regarding their website Petition notification (reproduced above) which page pointed out just some of the dangers of CBT (and GET) to ME and FM patients.
We have reproduced below the letter we sent to Clwyd, and others, asking direct questions about the page, but noting also recent evidence we had located showing further that both N Wales NHS Clinics were operating together under exactly the same psychotherapeutic auspices and rational; something Clwyd Group had ardently denied over many previous years despite other evidence we provided and shall declare in these notes at a later stage.
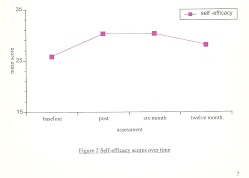
In the first four years of their operations, the N Wales Clinics had used self-reporting patients undergoing CBT/GET to generate data, analysed by a University of Bangor statistics department (IMSCAR), to provide evidence for the so-called efficacy of their psychological-behavioural approach to CFS/ME FM patients. The claim was made by the Clinics that such evidence had thus been demonstrated.
We brought the further evidence and facts to Clwyd’s attention also, and can let our letter speak for itself:
"Questions have been asked of the NWW ME/FM Support Group Committee regarding a continuing Clwyd Group web page that has invited individuals to participate in a vote against Clinics practicing psychological CBT methods of intervention for our patients, and based on psychiatric approaches promoted by practitioners such as Simon Wessely.
The Clwyd web page correctly suggests that, ‘CBT is a tool used for mental illness, a category inapplicable to ME and FM. These conditions are organic, not psychosomatic, and patients can be caused more harm than good with these methods; their condition can be made worse, in fact.
And patients can be stigmatised for life (by friends, family, associates, employers, and GPs) as ‘psychiatric.’ Benefits, too, may be compromised or lost. Appropriate Research is hindered into the immuno-neurological correlates of CFS/ME, evident in the many Research findings, and by the WHO definition.’
(our paraphrase)
What the Clwyd petition does not appear to note is that both North Wales CFS/ME/FM Clinics are Wesleyan CBT psychiatric Services, the very cause for alarm that has been made repeatedly over the years by the NW Wales Support Chair, as well as the Founding Chair of WAMES, Ian McDonald.
On one occasion, for example, we made it clear that pooled Statistical Results for the Clinics, as were produced in their first years of operations, have to represent methodologies that are identical at both Services.
This fact (in the statistical sciences) was rejected by Clwyd who continued to maintain that if the NW Wales Clinic was having problems, ‘the two Services must be running differently.’ This abject denial of the reality was not true then and it is still not true today. There are many other examples of this unremitting support for the Flintshire CBT psychiatric Clinic by Clwyd group over the years.
Bangor University IMSCAR Evaluation of the two Welsh Clinics (sat on and buried for four years following our accurate criticism of it, and now accessed) states:
“The North Wales Chronic Fatigue Service was established in April 1999…The approach is based on a cognitive behavioural model…CBT is based on a biological psychosocial conceptualisation of the patient’s problems and includes psychotherapeutic, informational, behavioural and problem solving components.
A cognitive behavioural model of CFS assumes that illness related beliefs and cognitions play a CENTRAL ROLE in CFS and these beliefs in turn influence a person’s emotional and PHYSIOLOGICAL STATE...."
(- Our emphasis)
Translating this 'CBT-talk'
‘perpetuating, archaic, inappropriate and non functional mental beliefs and sickness behaviours, surrounding the patient’s misconstrued health status and circumstances, promote the emotional and physiological states and symptoms in CSF/ME and FM patients. Patients are not so ill as at least they think they are in their fixated cognitions which they’ve come to believe and act out behaviorally, reinforcing the very physiological states they complain of.’
These conditions are therefore ‘psycho-somatic’ (mind to body) - the very thing the Clwyd page maintains ME/FM is not.
And, to illicit support for these damaging contentions, the Report’s References page points our patients, carers, GPs and researchers to such authors as are renown in ME/FM and GWS circles: to Chandler, Sharpe and Simon Wessely, as sources of both N Wales Clinic’s authority and rational.
Will Clwyd now either publicly renounce its longstanding and tenacious protection, backing and active promotion of its Wesleyan CBT psychiatric Clinic in Flintshire, and their methods, or will it maintain its web Petition notification to the world denouncing such Clinics but, then, explain its duplicity?
The amount of serious damage both these Clinics have been able to visit on our patients over years now in N Wales is only hinted at on Clwyd’s Petition page. We have reasoned, barracked, pleaded and yelled about what we have seen and known for nine years now, unheeded by Clwyd, while ME/FM patients by the hundreds, right across North Wales, went to the wall year after year.
How can Clwyd Group, following its unremitting support of the CBT Clinics (and WAMES with its liability of ‘sanctioning-by-silence’) redress those damaging consequences that its web page speaks of, to some 1,000 of our ME/FM patients by now since 1999 (if we include the many victims left without any help whatever - those turned down by the Clinics as ‘unsuitable’, or others too smart to sign-up for a psychiatric characterization of their illness)?
Will Clwyd apologise to them all, if it can ever locate even a fraction of the most of them? Or reimburse them for the ‘lost benefits’ that Clwyd notes? Shouldn’t some of its Committee think about resignation? But will that redress the many who have been ‘made worse’ and ‘stigmatised’, according to Clwyd’s own assessment, and by its own CBT/GET Clinic?
Alarming also is the realization that many other CBT Clinics, modelled on these two long-standing Services (wholly unchallenged for years by Clwyd and WAMES and therefore assumed by patients, carers, service providers, and all, to be exemplary), have consequentially proliferated widely across the UK, spreading CBT/GET for CFS/ME even further, and for tens of thousands now.
As we have noted above, the Petition Page did disappear some time later, and we wonder if by that Clwyd therefore no longer concurs that CBT is a danger to ME/CFS FM patients?
But what remains are two further important questions. Why, as we have here demonstrated, are Clwyd still promoting the two CBT/GET Clinics based on psychatric theorotician Simon Wessley’s proposals for treatment, and why after 2004 did the IMSCAR results suggesting that CBT/GET works for CFS/ME and FM patients in N Wales suddenly get buried?
........................................................................................................